ISSN: 1859 - 2872
ISSN: 1859 - 2872
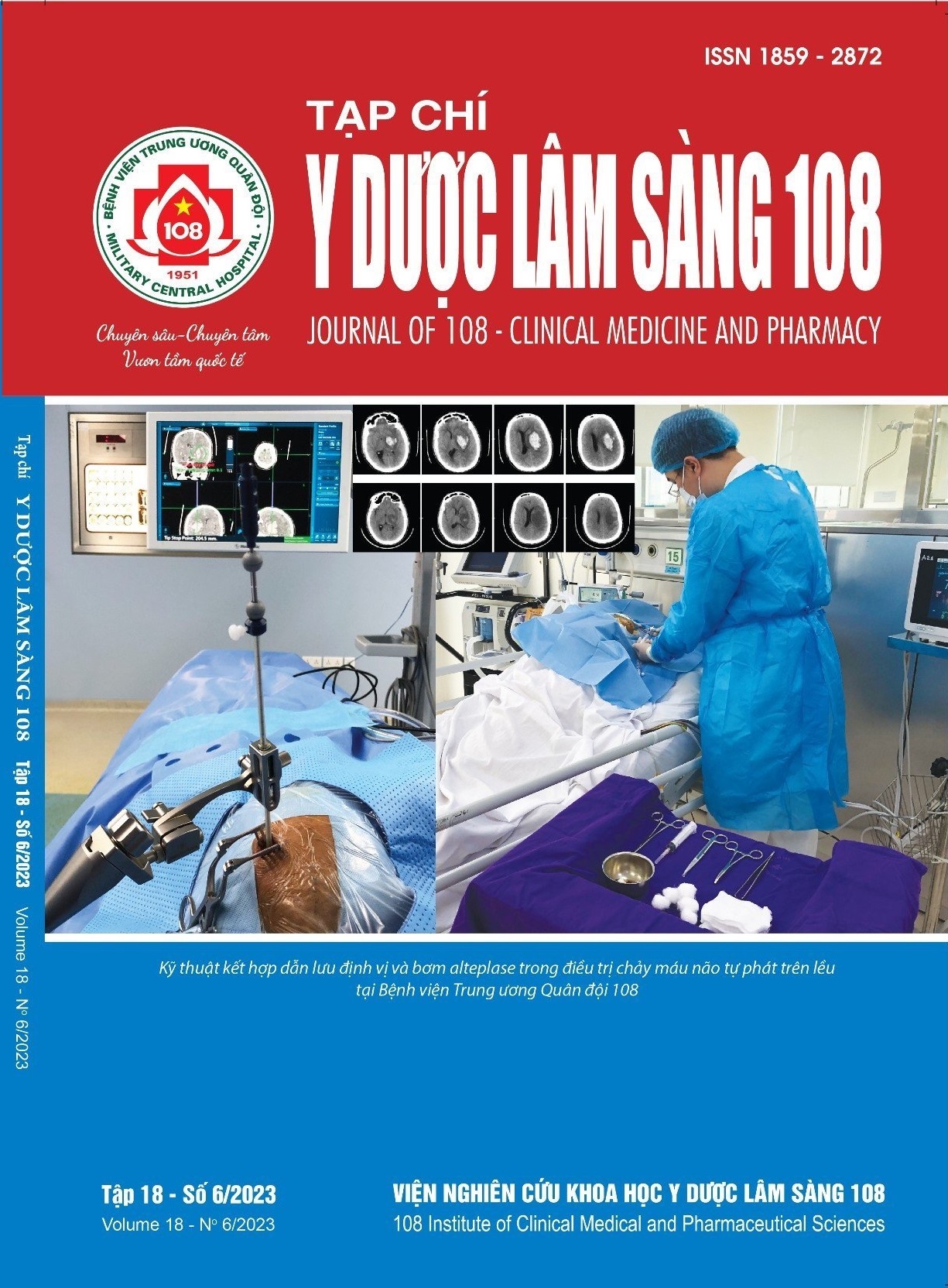
Early results of combined navigation guided drainage surgery with alteplase in treatment of spontaneous supratentorial intracerebral hemorrhage
Main Article Content
Keywords
Abstract
Objective: To evaluate results of navigation guided drainage surgery in combination with ateplase for spontaneous supratentorial intracerebral haemorrhage at hospital discharge. Subject and method: A prospective study of 80 cases spontaneous supratentorial intracerebral haemorrhage underwent frameless stereotactic aspiration the hematoma plus alteplase at 108 Military Central Hospital. Average age was 55.6 ± 11.4 (28-80), male/female was 4/1. Bleeding in the basal ganglia - thalamus was 73.7%. The mean hospital stay was 14.8 ± 5.7 days. Result: Conscious status at hospital discharge (Glasgow score) improved compared to preoperative (10.9 vs 8.9, p<0.05); hematoma volume decreased from 71.9 to 23.9ml; midline shift decreased from 10.6 to 5.6mm (p<0.01). Factors related to the state of consciousness at discharge include: Preoperative Graeb score (r = -0.34, p<0.01), postoperative residual hematoma volume (r = -0.49), p<0.01), degree of midline shift (r = -0.4, p<0.01) and Graeb score at discharge (r = -0.49, p<0.01). Conclusion: Navigation guided drainage surgery in combination with ateplase improved the clinical status according to the Glasgow scale, reduced hematoma volume, midline shift and Graeb score. The smaller the remaining hematoma volume, the better the patient's improvement.
Article Details
References
2. Li M, Mu F, Su D, Han Q, Guo Z, Chen T (2020) Different surgical interventions for patients with spontaneous supratentorial intracranial hemorrhage: A network meta-analysis. Clin Neurol Neurosurg 188: 105617.
3. Broderick JP, Brott TG, Duldner JE, Tomsick T, Huster G (1993) Volume of intracerebral hemorrhage. A powerful and easy-to-use predictor of 30-day mortality. Stroke 24(7): 987-993.
4. Liao CC, Chen YF, Xiao F (2018) Brain midline shift measurement and its automation: A review of techniques and algorithms. Int J Biomed Imaging 2018: 4303161.
5. Graeb DA, Robertson WD, Lapointe JS, Nugent RA, Harrison PB (1982) Computed tomographic diagnosis of intraventricular hemorrhage. Etiology and prognosis. Radiology 143(1): 91-96.
6. Sirh S, Park HR (2018) Optimal surgical timing of aspiration for spontaneous supratentorial intracerebral hemorrhage. J Cerebrovasc Endovasc Neurosurg 20(2): 96-105.
7. Yang X, Zhu Y, Zhang L, Wang L, Mao Y, Li Y, Luo J, Wu G (2021) The initial CT blend sign is not associated with poor patient outcomes after stereotactic minimally invasive surgery. BMC Neurol 21(1): 160.
8. Teernstra OP, Evers SM, Lodder J, Leffers P, Franke CL, Blaauw G; Multicenter randomized controlled trial (SICHPA) (2003) Stereotactic treatment of intracerebral hematoma by means of a plasminogen activator: A multicenter randomized controlled trial (SICHPA). Stroke 34(4): 968-974.
9. Wang WZ, Jiang B, Liu HM, Li D, Lu CZ, Zhao YD, Sander JW (2009) Minimally invasive craniopuncture therapy vs. conservative treatment for spontaneous intracerebral hemorrhage: Results from a randomized clinical trial in China. Int J Stroke 4(1): 11-16.
10. Polster SP, Carrión-Penagos J, Lyne SB, Goldenberg FD, Mansour A, Ziai W, Carlson AP, Camarata PJ, Caron JL, Harrigan MR, Gregson B, Mendelow AD, Zuccarello M, Hanley DF, Dodd R, Awad IA (2021) Thrombolysis for evacuation of intracerebral and intraventricular hemorrhage: A guide to surgical protocols with practical lessons learned from the MISTIE and CLEAR trials. Oper Neurosurg (Hagerstown) 20(1): 98-108.
Article Sidebar